Unmasking the ACEs, and Helping Students Manage their Emotions in School
Dear Colleagues,
Introduction
The new school year started this week in many districts across the country. And many of the administrative and faculty workshops and discussions that I have led this month, in before-school trainings and institutes, have focused on school climate and school safety.
And rightly so.
Immediately after the El Paso and Dayton slaughters just weeks ago, different U.S. news agencies reported the number of mass shooting so far this year as between 17 (ABC News) and 255 (HuffPost—which defines a mass shooting as one where at least four people are shot).
Relative to children and adolescents under the age of 17, the non-profit Gun Violence Archive, which maintains an incident-specific data-base on its website, reports that so far this year (a) there have been 261 mass shootings (more occurred after Dayton); (b) 420 children between the ages of 0 and 11 years old have been killed or injured by gun violence; and (c) 1,923 adolescents between 12 and 17 years of age have additionally been killed or injured by gun violence.
To put these numbers into context, past Center for Disease Control and Prevention reports (one published in the journal Pediatrics in 2017) estimate that approximately 50% of all gun-related deaths involving children and adolescents each year are homicides, and one-third are suicides.
The bottom line is: Students and staff across this country are returning to school this year more concerned about (gun) violence and the threat of (gun) violence at school and in their communities than ever before.
_ _ _ _ _ _ _ _ _ _
Beyond Anxiety Over Gun Violence: The Current State of Trauma-Sensitive Programs
As noted above, given all of this community-based violence (and other incidents of violence that are family- or peer-based), many students are coming to school this new year especially impacted by trauma. While many schools are adopting “trauma-sensitive” strategies, it is important for educators to understand the important psychological facets of trauma so that they implement approaches that are timely, effective, and worthwhile.
Critically, if schools are implementing generic, off-the-rack trauma-sensitive “packages” that are not individualized to their students, staff, and school community, the packages are unlikely to be timely, effective, and worthwhile. In fact, they may counterproductively increase some students’ trauma (think an active shooter drill in school that always increases some students’ and staff members’ anticipatory trauma).
One problem is that the trauma-sensitive schools “movement”—largely initiated by the Adverse Childhood Experiences (ACEs) study—has created a “cottage industry” of “experts and consultants” who have created their own (what they call) “research-based trauma programs.”
Unfortunately, many of these programs have never been fully and objectively field-tested (if at all). . . in multiple settings, under multiple conditions, and with students who have experienced different types and intensities of trauma.
Said a different way: While many of these programs cite research that explains why they have included certain components or activities, they have not—themselves—been researched.
In fact, even from a research perspective, many of these programs are not psychologically and neuropsychologically grounded. That is, they do not use the "deep science” of trauma—including the clinical, multi-tiered psychoeducational elements needed for student and staff success.
Moreover, many of these programs are “stand alone” programs. They do not integrate their approaches into the school’s existing discipline, behavior management, and student self-management systems, and they often are seen by staff as a disconnected thread of information that represents “another thing to do” . . . in an already impossibly busy day, week, and month.
Finally, too many of these programs recommend global and generic components and activities that are not strategically-chosen or sustainable. The programs present a fixed package. . . rather than presenting sound strategies on how to identify and then analyze the root causes of students’ trauma— so that the assessment results can be strategically linked to needed services, supports, and interventions.
Part of this latter problem exists because many educators do not fully understand the history and limitations of the original ACEs research, and they do not have the psychological understanding to discriminate potentially effective from ineffective trauma-sensitive practices.
Indeed, some educators are focused more on program or package implementation, rather than effective and strategically-selected trauma-responsive practices.
_ _ _ _ _ _ _ _ _ _
What the ACE Research Is and Isn’t
The original ACE Study was conducted by the Kaiser Permanente Health Maintenance Organization (HMO) in Southern California from 1995 to 1997 with two waves of data collection. As they were receiving physical exams, over 17,000 HMO members completed confidential surveys regarding their childhood experiences and their current health status and behaviors. Significantly, beyond the fact that the sample was from a limited geographic area, the participants were primarily white and from the middle class.
Below are the actual ACE Study Questions. Each “Yes” response received one point toward the “final score.” As educators, please read these items relative to today’s students. Think about how many of your students have experienced four or more of these events so far in their lives (more on that below).
While you were growing up, during your first 18 years of life:
1. Emotional Abuse. Did a parent or other adult in the household often or very often… Swear at you, insult you, put you down, or humiliate you?
or Act in a way that made you afraid that you might be physically hurt?
2. Physical Abuse. Did a parent or other adult in the household often or very often… Push, grab, slap, or throw something at you?
or Ever hit you so hard that you had marks or were injured?
3. Sexual Abuse. Did an adult or person at least 5 years older than you ever…
Touch or fondle you or have you touch their body in a sexual way?
or Attempt or actually have oral, anal, or vaginal intercourse with you?
4. Emotional Neglect. Did you often or very often feel that … No one in your family loved you or thought you were important or special?
or Your family didn’t look out for each other, feel close to each other, or support each other?
5. Physical Neglect. Did you often or very often feel that … You didn’t have enough to eat, had to wear dirty clothes, and had no one to protect you?
or Your parents were too drunk or high to take care of you or take you to the doctor if you needed it?
6. Parental Separation or Divorce. Were your parents ever separated or divorced?
7. Mother Treated Violently. Was your mother or stepmother: Often or very often pushed, grabbed, slapped, or had something thrown at her?
or Sometimes, often, or very often kicked, bitten, hit with a fist, or hit with something hard?
or Ever repeatedly hit at least a few minutes or threatened with a gun or knife?
8. Household Substance Abuse. Did you live with anyone who was a problem drinker or alcoholic or who used street drugs?
9. Household Mental Illness. Was a household member depressed or mentally ill, or did a household member attempt suicide?
10. Incarcerated Household Member. Did a household member go to prison?
_ _ _ _ _
The most critical concerns with the ACEs’ Questions are:
- They do not discriminate between “finite” events (e.g., having a household member incarcerated) and events that can occur over time or in a repeated way;
- Thus, they do not quantify many of the events (e.g., how long was the separation, how many times was your mother physically threatened);
- They do not identify the age (or age range) when the child or adolescent experienced each event;
- They do not ask for a rating of the intensity of each event (e.g., along a Mild-Moderate-Severe continuum);
- They do not get a rating of the emotional impact of each event at the time that it occurred (e.g., along a None-Low-Mild-Moderate-Significant-Life Changing continuum); and
- They do not get a rating of the current (assuming an event occurred in the past) and/or continuing emotional impact of each event.
Given the absence of this critical contextual information, we do not really know the cumulative depth, breadth, intensity, or impact of an individual’s traumatic history. Indeed, we may just simply know how many events an individual may have experienced.
_ _ _ _ _
Briefly, the results of the original ACEs study indicated that:
- About two-thirds of participants reported at least one adverse childhood experience;
- The number of ACE points were strongly associated with high-risk health behaviors during adulthood such as smoking, alcohol and drug abuse, promiscuity, and severe obesity;
- The number of ACE points also correlated with depression, heart disease, cancer, chronic lung disease, and a shortened lifespan.
- Compared to an ACE score of zero, having four adverse childhood experiences (i.e., Four or more ACE points) was associated with a seven-fold (700%) increase in alcoholism, a doubling of risk of being diagnosed with cancer, and a four-fold increase in emphysema; and
- An ACE score above six was associated with a 30-fold (3,000%) increase in attempted suicide.
More than 50 ACE-related studies have followed the original. These studies have (a) used more diverse and different participant samples—including children and adolescents as respondents; (b) looked at different physical, behavioral, mental health, and life outcomes; (c) adapted the original ACE survey and methodology; and (d) replicated many of the correlational (not causal) results from the original study.
In addition, the concerns highlighted by these studies resulted—starting in 2011 in Florida—in communities beginning trauma-awareness programs; and—about 10 years ago in Massachusetts, Washington, and California—in schools beginning similar trauma-related initiatives.
Relative to prevention, a 2016 Center for Disease Control and Prevention Monograph made the following recommendations:
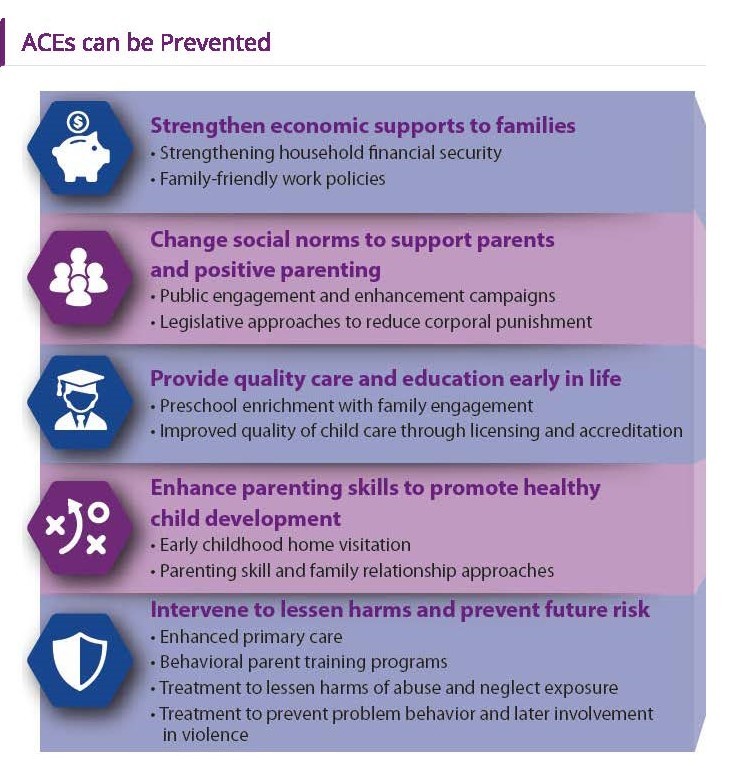
[CLICK HERE for More ACEs Information from the CDC]
But there still is not a well-established and validated science-to-practice foundation that connects the ACEs study with an effective approach to trauma awareness and programming in the schools. The closest we get is an October, 2018 report by the American Institutes for Research (AIR; more on this report below), Trauma and Learning Policy Initiative (TLPI): Trauma-Sensitive Schools Descriptive Study.
_ _ _ _ _ _ _ _ _ _
A Science-to-Practice Foundation to Trauma Programming in Schools
Quite honestly, as discussed in the Introduction to this Blog message, we do not need—in 2019—the ACEs study to tell us that some students come to school having experienced significant emotional traumas in their lives, or that all schools need to create and sustain safe school climates and positive, supportive classrooms. Moreover, to a large degree, the neurophysiological and neuropsychological pathways and impact of trauma have been known for many years.
But, to their credit, what the ACEs and follow-up research studies have done is to crystallize the discussion and information, and put it directly in the hands of different educators—helping them to better understand some of the social, emotional, and behavioral interactions of our children and adolescents.
But we may have gone too far, too fast in specializing our quest to create “Trauma-Sensitive Schools.”
Indeed, in the first paragraph of the Executive Summary of AIR’s Trauma-Sensitive Schools Descriptive Study, the authors state:
Background and Introduction:
School Climate and Culture and School Improvement
For decades, educators and policymakers have grappled with the issue of school improvement—or how to create systemic changes that lead to better and sustained student academic outcomes. A growing body of evidence suggests that school improvement efforts cannot happen without considering the impact of school climate and culture. Research demonstrates that a positive school climate (which includes factors such as safety, a sense of connectedness and belonging, social and emotional competencies, and the physical environment) is associated with positive student outcomes (Kraft, Marinell, & Yee, 2016; Kwong & Davis, 2015). Specifically, a positive school climate is associated with higher student achievement, improved psychological well-being, decreased absenteeism, and lower rates of suspension.
It also has been found that improving safety and school climate can help reduce bullying and aggression (Bradshaw, Mitchell, & Leaf, 2010; MacNeil, Prater, & Busch, 2009; Ross & Horner, 2009; Thapa, Cohen, Guffey, & Higgins-D’Alessandro, 2013). In addition, research indicates that the perception of a positive school climate, though beneficial for all students, may be even more useful for students at risk for negative outcomes (Loukas, 2007). The latter finding is particularly important given the prevalence of trauma among students in schools.
While the remainder of the 118-page report focused on the impact of trauma—because AIR was being paid to produce this report for a trauma-focused educational organization—the paragraph above reflects the appropriate mindset that all educators must have when even considering a trauma-sensitive program.
That mindset should be:
Focus on establishing and sustaining prosocial and safe school climates, and positive and supportive classrooms interactions.
As part of this school discipline, classroom management, and student self-management process, identify how trauma—and other critical factors—are affecting students’ social, emotional, and behavioral readiness for and interactions in school, and integrate prevention and early-response services, supports, and strategies to address high-hit circumstances or needs.
For students with significant social, emotional, behavioral, or mental health needs (whether trauma-based or not), schools need a multi-disciplinary team of diverse experts who can analyze the root causes of the problems, and link the assessment results to effective, research-based multi-tiered services, supports, strategies, and interventions.
In other words, the mindset should be one where educators are establishing comprehensive, evidence-based, multi-tiered school discipline (or positive behavioral support/social-emotional learning) systems that integrate trauma as but one factor affecting students’ behavior, interactions, and academic readiness and engagement.
Moreover, this suggests that schools should not implement a dedicated Trauma-Sensitive Program as its core (or even secondary) system relative to schoolsafety and discipline, classroom climate and management, and student self-management and academic engagement.
This is because:
- A Trauma-Sensitive Program may be too specialized for the typical school, and it may miss many of the non-trauma factors that contribute to school safety and climate;
- The Trauma-Sensitive Program may not be needed (thus, saving time, training, money, and motivation) if trauma-related information and practices are integrated into the core system;
- Most Trauma-Sensitive Programs are not even close to addressing the (Tier II and Tier III) strategic or intensive multi-tiered needs to specific students; and
- We still do not have a sound research-to-practice foundation (as discussed above) to know which trauma-sensitive practices and interventions provide the best services and supports to students, and the best return-on-investment to schools.
_ _ _ _ _
If you are interested in the results of the AIR trauma-sensitive schools study:
[CLICK HERE for the Full Report]
Understand, however, that this Report is a qualitative (not quantitative) study, and that it focused on the experiences of only five schools. Moreover, the purpose of the AIR study was to understand how an inquiry-based process was useful in supporting the educators in the five participating schools to transform their school’s culture to become more trauma sensitive. More specifically, they studied how a systems-level process helped educators to shift their thinking, deepen their understanding, and change their practices relative to the impact of trauma on learning.
Critically: The AIR Report was not about what multi-tiered services, supports, strategies, and interventions had the greatest impact on helping students to minimize the impact of trauma on their social, emotional, or behavioral interactions. The Report focused on how to build a systemic infrastructure for change.
And while it provides some sound advice, professionals should use that advice to strengthen the organizational development and buy-in to their core school discipline, classroom management, and student self-management system.
And so, in the context of the mindset recommendation above, professionals who decide to read the AIR Report should substitute the words, “School Safety, Climate, and Discipline” for “trauma” or “trauma-sensitive” as they read the Report.
And, educators who are interested in the evidence-based components and specific multi-tiered services, support, strategies, and programs needed for your core system:
Feel free to download our free monograph, Project ACHIEVE’s School Improvement and Positive Behavioral Support System/Social-Emotional Learning Overview
[CLICK HERE and Find at the Bottom of the Page]
and consider its companion resource, A Multi-Tiered Service and Support Implementation Guidebook for Schools: Closing the Achievement Gap
[CLICK HERE and Find at the Top of the Page]
At this point, however, let’s discuss one of the critical elements in helping students to manage their emotions— whether they are trauma-related or triggered in other ways.
_ _ _ _ _ _ _ _ _ _
The Science-to-Practice Components of Emotional Self-Management
Last month (July 16, 2019), Education Week reported on a teacher survey that its Research Center conducted with classroom teachers relative to how prepared and supported they felt in addressing their students’ significant social-emotional needs.
[CLICK HERE for the Education Week article]
Relative to our discussion here, the critical “take-aways” were:
- While most of the teachers responding to the survey said it's important to teach social-emotional skills, many still don't feel equipped to help students manage their emotions—especially when it comes to the children who are demonstrating the greatest needs.
- Indeed, 43% of the teachers said they had difficulty "finding ways to help students who appear to be struggling with problems outside of school."
- 23% of the teachers said that their most challenging task was "finding ways to help students who appear to be experiencing emotional or psychological distress."
- Less than 40% of the surveyed teachers said they received training in conflict de-escalation, a similar number reported training in child trauma, and only 29% reported receiving mental health training.
- Some teachers above said that their training did not cover practical, classroom-based strategies for the more complicated, emotional, severe, or dangerous student situations they might experience.
- When faced with these significant problems, most of the teachers turned to school-based professionals like psychologists or counselors. But almost 50% of all the surveyed teachers reported that they could not call on these staff members when they needed them.
- Indeed, 46% of respondents said they "somewhat" or "completely" disagreed that “their school had adequate support services from counselors, school psychologists, or other professionals to assist students experiencing emotional or psychological distress.”
- Thus, 70% of the teachers said they addressed their students' mental-health challenges by talking with them themselves.
_ _ _ _ _
The Emotional Self-Management Components: Teachers, Support Staff, and Students
One of the ultimate goals of a comprehensive school discipline (Positive Behavioral Support/Social-Emotional Learning, PBSS/SEL) system is to teach and motivate students to learn, master, and independently apply social, emotional, and behavioral self-management skills. Emotional self-management skills, which some call “emotional self-regulation” or even “emotional intelligence,” involves instruction in emotional awareness, emotional control, and emotional coping skills.
Below are the psychological and neuropsychological science-to-practice elements that we alluded to earlier in this Blog message. Remember, we noted that these elements are often missing in many “trauma-sensitive” programs.
Emotional awareness involves (a) students’ identification, knowledge, understanding, and discrimination of the many different emotions that they may experience in their lives; (b) their awareness of the emotional triggers that exist in the settings that they go to or must attend; (c) their awareness of their physiological cues and responses to different emotional situations; and (d) their awareness of how others look and act when they are in different emotional situations or states.
Emotional control occurs when students are able to maintain (a) the physiological control of their bodies when under conditions of emotionality, so that (b) they are able to think clearly and rationally—demonstrating effective social problem-solving skills, so that (c) they can demonstrate appropriate social interactions and behavioral self-management skills.
Emotional coping goes beyond the emotional control that occurs when students are experiencing emotional conditions “in the moment.” Emotional coping occurs as students are debriefing and reconciling a just-past emotional situation, or are learning to minimize the impact of a persistent or emotionally traumatic situation. Ultimately, emotional coping skills help students to (continue to) live their lives in emotionally positive and healthy ways—even in the face of continuing, similar, or new traumatic situations (or those that trigger emotional memories).
_ _ _ _ _
When students are taught these components—from preschool through high school—they are more able to handle the emotional triggers in their lives. Critically, though, the instruction starts in the general education classroom, taught by students’ classroom teachers. The anchor to this instruction is an evidence-based social skills curriculum that literally teaches students—at their specific developmental level—emotional control, attributional and attitude control, and behavioral execution skills.
Like literacy, math, and writing, this curriculum should be a core responsibility of the classroom teacher, and a planned part of the instructional week. And, like literacy, math, and writing, classroom teachers should receive comprehensive instruction and coaching so that they are skilled and comfortable in delivering this curriculum with integrity.
Moreover, they should be supported by the mental health and related service professionals in their schools (e.g., school psychologists, counselors, and social workers). These professionals should be part of the “coaching team,” they should be available to co-teach some of the curriculum as needed, and—most critically—they should be working in small groups and individually with students who need more strategic or intensive attention.
Indeed, some of the clinical interventions that may be needed at this deeper multi-tiered level include:
- Progressive Muscle Relaxation Therapy and Stress Management
- Emotional Self-Management (Self-awareness, Self-instruction, Self-monitoring, Self-evaluation, and Self-reinforcement) Training
- Emotional/Anger Control and Management Therapy
- Self-Talk and Attribution (Re)Training
- Thought Stopping approaches
- Systematic Desensitization
- Trauma-Focused Cognitive Behavioral Therapy (TF-CBT)
- Cognitive-Behavioral Intervention for Trauma in Schools (CBITS)
- Structured Psychotherapy for Adolescents Responding to Chronic Stress (SPARCS)
- Trauma Systems Therapy (TST)
The Question is: Do your related service professionals have the skills to clinically deliver (as needed—based on student-centered assessments) some or all of these strategies or therapies. . . or, are they available from mental health professionals who are practicing in your community?
_ _ _ _ _
Developmental Differences and Students’ Emotional Triggers
Part of the emotional control training also involves a recognition of the developmental differences of students from preschool through high school. Another part involves an understanding of students’ shared and individual emotional triggers.
Relative to the former area, there are significant developmental and emotional differences between students at the preschool to Grade 2, Grades 3 to 5, and Grades 6 and above levels. Teachers need to factor these differences into their classroom self-management discussions and instruction—both as they plan and as they implement the social skills curriculum.
At the preschool to Grade 2 level, students are concrete, sequential, and egocentric in their thinking. Early on, they don’t even have an emotional vocabulary to help them identify or express their feelings. Later on, they are egocentrically focused more on their own—than others’—feelings, and their insight is limited relative to the social complexities of many interpersonal situations. Given all of this, then, teachers at these grade levels will need to be both their students’ social, emotional, and behavioral guides, as well as their emotional control prompters and compasses.
At the Grade 3 to 5 level, students are beginning to develop higher-ordered thinking skills (both academically and behaviorally), they have more self-insight, and they are more able to predict and understand how others are feeling. . . and why they are reacting in different social situations. At these grade levels, however, teachers still need to teach their students about their own and others’ feelings, and how to analyze and solve common social situations. In other words, while students here are more developmentally ready to solve more complex social situations and dilemmas, they still need the instruction.
An academic parallel here is when Grade 4 students are more cognitively ready to handle abstract and multi-level comprehension questions in literacy or science, but they still need the instruction in how to do this.
At the Grade 6 and above level, students’ emotional situations are compounded by their desire for more independence, physiological and sexual changes, enhanced academic and organizational demands, the impact and influence of different peer groups, and their less restricted exposure to social media, internet-driven, and news or entertainment broadcasts and events that touch on sensitive issues or ones they have yet to experience.
Here, teachers need to recognize that, while they often “sound” mature, these students still need training and guidance in (a) how to handle these complex or sensitive social situations; (b) how to communicate in or respond to highly emotional personal, peer, or adult situations; (c) how to understand and navigate their virtual, social media-driven worlds; and (d) how to integrate moral and ethical decision-making into these social dilemmas and deliberations.
Critically, this requires a blend of advanced skill instruction, group discussion and processing, social problem-solving simulations, and personal reflection and self-evaluation.
_ _ _ _ _
Relative to the latter area, students’ emotions are triggered in many different ways.
While they are a good start, the issues embedded in the ACEs questions (revisit them above) need to be expanded, as relevant, to community, school, and peer experiences and interactions. To reflect this, below is a table with the original ten ACEs areas, with X’s in the boxes where these traumas could also occur in non-familial settings or with individuals who are not family members.
The point here is that: These events or issues are no longer limited to our students’ familial experiences, and our trauma-related assessments need to include these multiple settings. Said a different way: “Trauma is not setting-specific. It is event-dependent.” Traumas obviously can be experienced outside of the “family home,” and be just as emotionally debilitating.
Source: Trauma: | Family/Extended Family (Original ACEs) | Community | School | Peers |
Physical Abuse | X | X | X | X |
Verbal Abuse | X | X | X | X |
Sexual Abuse | X | X | X | X |
Physical Neglect | X | X | X | |
Emotional Neglect | X | X | X | |
Alcoholism/(Drugs) | X | X | X | X |
(Domestic) Violence | X | X | X | X |
Incarceration | X | X | ||
Mental Illness | X | X | X | X |
Divorce, Death, or Abandonment | X | X | X | X |
But beyond the trauma areas above, other areas that trigger students’ emotionality include:
- Academic Frustration
- Test/Homework/Work Completion Anxiety
- Peer (including Girlfriend/Boyfriend) Conflicts/Rejection
- Teasing and Bullying—Direct, Indirect, Social, and Social Media
- Gender Status or Discrimination
- Racial or Multi-Cultural Status or Discrimination
- Sexual Identification or Orientation Discrimination
- Socio-economic Status or Discrimination
- Circumstances Related to Poverty/Parental Income
- Family Moves/Housing Mobility/Homelessness
- Competition/Losing
- Physical or Other Limitations or Disabilities
On a situational level, these triggers can product emotional reactions that are just as quick and intense as those that are trauma-related, and these need to be consciously factored into a school climate, discipline, and classroom management system.
Moreover, as in the trauma research, please remember that student emotionality can be manifested along a “fight, flight, or freeze” continuum.
The Take-Aways here, once again, include the following:
- There are multiple circumstances or events that trigger students’ emotionality in school. Many of them are not specifically (or by definition) traumatic events and, thus, schools that are using trauma-sensitive programs may easily miss them.
- Schools need to assess and identify the emotional triggers that are most prevalent across their student bodies, and the emotional triggers (if different) that are most often present for the students presenting with the most frequent, significant, or severe social, emotional, and behavioral challenges.
- For the former group, these triggers need to be integrated into the social skills curriculum at the prevention and early response levels.
- For the latter group, these triggers need to frame the strategic or intensive interventions or therapies that related services personnel need to be prepared to deliver.
- Finally, schools and districts need to be prepared to deliver the full multi-tiered continuum of services, supports, strategies, and interventions. This includes the necessary training, resources, and personnel both in general, and as needed on a year-to-year basis.
_ _ _ _ _ _ _ _ _ _
Summary
We started this Blog “journey” by discussing how students and staff across the country are returning to school this year more concerned about (gun) violence and the threat of (gun) violence at school and in their communities than ever before.
The discussion then moved to a recognition that “trauma sensitive school programs” are still in their infancy, that most of them have not been field-tested nor independently proven to be effective in multiple settings and under multiple conditions, and that—if implemented—these programs will not address the comprehensive emotional needs of most students as there are many emotional triggers that are not trauma-related.
Next, we addressed the reality and limitations of the original late-1970s ACEs research, and concluded that:
- Schools need to focus on establishing and sustaining prosocial and safe school climates, and positive and supportive classrooms interactions.
- As part of this school discipline, classroom management, and student self-management process, they need to identify how trauma—and other critical factors—are affecting students’ social, emotional, and behavioral readiness for and interactions in school, and integrate prevention and early-response services, supports, and strategies to address high-hit circumstances or needs.
- For students with significant social, emotional, behavioral, or mental health needs (whether trauma-based or not), schools need a multi-disciplinary team of diverse experts who can analyze the root causes of the problems, and link the assessment results to effective, research-based multi-tiered services, supports, strategies, and interventions.
- And so, all of this suggests that schools should not implement a dedicated Trauma-Sensitive Program as its core (or even secondary) system relative to school safety and discipline, classroom climate and management, and student self-management and academic engagement.
We concluded the discussion by outlining the components needed in the recommended multi-tiered system that integrates trauma-relevant incidents and issues, and specifying what teachers need to do, and what related services professionals should be prepared to do.
All of this is focused on helping schools to most effectively address the social, emotional, and behavioral needs of all students—with a focus on their emotional self-management. When students have emotional self-management skills, and the support around them to facilitate emotional control and coping, issues related to trauma and emotional triggers become less evident, because most everyone is “handling” them.
Our schools still have a ways to go. We need to be mindful of the recent Education Week survey. If teachers don’t have the (right) training, professional development, and support; and if they don’t have the trained and available mental health and related service colleagues available, these gaps will (continue to) undermine all of the best intentions, plans, and initial steps.
_ _ _ _ _
As always, I look forward to your thoughts and comments.
With the new school year beginning, I am always available to provide a free hour of telephone consultation to those who want to discuss their own students, school, or district needs. Feel free to contact me at any time if there is anything that I can do to support your work. . . now, and as you enter this new school year.
Best,