Understanding Seizure Types, Causes, and Connections to Stress and Brain Injury
Connecting Students’ Sensory and Neurological Functioning with School Learning, Socialization, and Disabilities (Part III)
Listen to a summary and analysis of this Blog on the Improving Education Today: The Deep Dive podcast on Spotify.
Hosted by popular AI Educators Angela Jones and Davey Johnson, they provide enlightening perspectives on the implications of this Blog for all of Education.
[CLICK HERE to Listen to this Popular Podcast]
(Follow this bi-monthly Podcast to receive automatic e-mail notices with each NEW episode!)
Dear Colleagues,
Introduction: We Start in the Supreme Court
Late last month (April 28, 2025), the Supreme Court heard the case, A.J.T. v. Osseo Area Schools, Independent School District No. 279 (No. 24-249). The case involves Ava Tharpe, a now-teenaged student with severe epilepsy and cognitive impairment against the Osseo Area Schools where she lived in Minnesota.
Ava has Lennox-Gastaut Syndrome, a severe form of epilepsy. This condition causes frequent seizures that are often resistant to medication, cognitive impairments that affect learning and communication, and developmental delays that require special education support.
When she was much younger, Ava attended a public school in Kentucky, where her schedule was adjusted to accommodate her debilitating condition. Specifically, her school arranged for her to attend classes only in the afternoon, and she also received instruction at home in the early evening.
When Ava’s family was preparing to move to Minnesota in 2015—Ava was in fourth grade—they consciously chose to move into the Osseo Area Schools community because the district agreed to match her school schedule and special education services.
After the move, however, the Osseo Area Schools refused to provide Ava’s services outside of the school day, denied her other accommodations, and reduced her school hours to about 65% of what her peers received.
Ava’s family sued the district, arguing that it failed to meet her Section 504 of the Rehabilitation Act of 1973 rights as a student with a disability. Specifically, she was being denied her equal access to the educational opportunities offered by the School District to other students.
After numerous lower and district court hearings and decisions, Ava’s case rose to the Supreme Court to clarify the legal standard for disability discrimination claims (and monetary awards) in education. On one side, the school district argued for a stricter standard requiring proof of "bad faith or gross misjudgment" as the criterion for discrimination, while Ava’s lawyers advocated for a more accessible "deliberate indifference" standard.
The issue for this Blog is not the impending Supreme Court decision—even though it will be significant regardless of how the Court rules.
The issue, given the theme of this Blog Series, is the importance that schools understand the different types of seizures that some students experience, and how to best accommodate and educate them relative to their academic learning and social development.
Recapping this Blog Series
This three-part Blog Series has focused broadly on three clusters of biologically-based conditions and their impact on students’ academic and/or social, emotional, or behavioral learning, interactions, and success.
Part I of this Blog Series discussed the wide assortment of disabilities that qualify students for services either under Section 504 of the Rehabilitation Act of 1973 or the Individuals with Disabilities Act (IDEA, 2004), respectfully.
Connecting Students’ Sensory and Neurological Functioning with School Learning, Socialization, and Disabilities: A Primer on Vision, Hearing, and Respiratory/Nasal Functioning (Part I)
_ _ _ _ _
In Part I, we noted that virtually every one of the 504 disabilities discussed—and virtually every one of the thirteen disabilities in IDEA—has an important relationship to the biological, physical or physiological, biochemical, or neuropsychological functioning of the students involved.
Moreover, we stressed that the different multi-disciplinary experts on every school’s 504, IDEA, or MTSS (Multi-Tiered System of Supports) team need to understand these biological-disability connections. . . from a curriculum, instruction, and learning perspective, as well as from an assessment, accommodation, and intervention perspective.
Finally, we emphasized that this expertise helps (a) create bridges between medical and educational professionals; (b) dismantles misconceptions that students with disabilities are simply choosing to be unsuccessful; (c) defuses beliefs that poor parenting, supervision, or motivation is to blame; and (d) promotes more empathetic and compassionate interactions by peers, staff, and administrators.
_ _ _ _ _
In the second Blog, we initially distinguished between headaches and migraines, and described how migraines affect students academically and socially in school.
Differentiating Headaches and Four Different Types of Migraines: Connecting Students’ Sensory and Neurological Functioning with School Learning, Socialization, and Disabilities (Part II)
_ _ _ _ _
We then discussed four types of migraines: Ocular/Retinal, Vestibular, Concussion-related, and Stress or Post-Traumatic Stress Syndrome migraines. We addressed their (a) common neurological, limbic, and biochemical structures and pathways; and (b) their distinct clinical presentations, neurobiological mechanisms, diagnostic considerations, and management approaches.
While educators do not differentially diagnose these four types of migraines, when interacting with students exhibiting them in school settings, they should still understand their clinical similarities and differences so that they can ask informed questions when conferring with parents and—with permission—medical professionals, and address students’ educationally-related needs.
Schools’ MTSS team members also need to understand the biological-disability connections discussed in this Blog Series. . . from a curriculum, instruction, and learning perspective, as well as from an assessment, accommodation, and intervention perspective.
_ _ _ _ _
In this third Blog in the Series, we will discuss the types and impact of seizures on students’ learning and engagement in school. We will especially focus on (a) the root causes and brain locations of the seizures covered; (b) the existence of Psychogenic Non-Epileptic Seizures (PNES)—formerly known as "pseudoseizures”—which often occur in individuals with trauma or abuse histories, but are not organic in origin; (c) how seizures themselves can contribute to PTSD and stress; and (d) the connection between seizures and traumatic brain injuries.
An Introduction to Seizures
Seizures are temporary disturbances in brain function that occur when there is abnormal electrical activity among brain cells. While many people associate seizures with convulsions or loss of consciousness, the reality is that seizures manifest in various ways depending on which part of the brain is affected. Understanding the different types can help with recognition, diagnosis, and proper management.
Seizures affect a significant number of students from kindergarten through Grade 12, with different frequencies by type. The most common types (discussed below) include absence seizures, which may go unnoticed as brief lapses in awareness; focal seizures, which affect specific areas of the brain and can cause unusual movements or sensations; and generalized tonic-clonic seizures, which involve full-body convulsions.
While exact numbers vary by region, studies estimate that approximately 1 in 100 children experience epilepsy, the condition most commonly associated with recurrent seizures. Among school-aged children, absence seizures are more frequent in younger students, while focal seizures and generalized tonic-clonic seizures are more commonly diagnosed in older students.
Critically, students with epilepsy often face difficulties beyond the seizures themselves. Compared to their peers, these students are more likely to:
- Miss 11 or more days of school per year;
- Require 504 or special education services;
- Experience learning difficulties, anxiety, and depression; and
- Face social stigma and peer bullying.
Schools play a crucial role in supporting students with seizure disorders by providing accommodations, emergency response plans, and education for staff and peers. These will be discussed toward the end of this Blog.
_ _ _ _ _
Describing the Different Types of Seizures
- Focal Seizures (Partial Seizures). Focal seizures originate in one specific area of the brain and can be subdivided into two main categories:
Focal Aware Seizures (Simple Partial) occur when the person remains conscious and aware during the event. They may experience unusual sensations like tingling, seeing flashing lights, smelling unusual odors, or experiencing sudden emotions.
These seizures are typically brief, lasting seconds to minutes, and often leave no confusion afterward.
_ _ _ _ _
Focal Impaired Awareness Seizures (Complex Partial) affect consciousness—the person may appear awake, but is not fully aware. Common behaviors include staring, and repetitive movements (automatisms) like lip-smacking, chewing, or hand rubbing. These seizures usually last 1 to 2 minutes, and are often followed by confusion.
_ _ _ _ _
- Generalized Seizures. Generalized seizures involve both hemispheres of the brain from the start and come in several types:
Absence Seizures (Petit Mal) present as brief lapses in awareness, often mistaken for daydreaming. They typically manifest as staring spells, sometimes with subtle eye or hand movements, lasting 5 to 30 seconds. Unlike other seizure types, there is no confusion afterward, and the individual can immediately return to normal activities. These seizures are most common in children.
_ _ _ _ _
Tonic-Clonic Seizures (Grand Mal) are the most recognized seizure type, featuring two phases. The tonic phase involves muscle stiffening, potential falls, and possible cries from air being forced out of lungs. The clonic phase follows with rhythmic jerking movements of limbs. These seizures usually last 1 to 3 minutes and are followed by confusion, fatigue, headache, and sore muscles.
_ _ _ _ _
Myoclonic Seizures involve brief, shock-like muscle jerks that may affect part or all of the body. They are typically very brief, lasting only seconds, and usually don't cause confusion afterward.
_ _ _ _ _
Atonic Seizures (Drop Attacks) cause sudden loss of muscle tone, resulting in abrupt falls or head drops that sometimes cause injuries. These seizures are very brief, lasting only seconds, and there is usually a quick recovery.
_ _ _ _ _
Tonic Seizures involve muscle stiffening without the clonic phase, often causing a rigid posture that can lead to falls if standing. These seizures usually last less than 20 seconds with a brief recovery period.
_ _ _ _ _
Clonic Seizures present as repetitive jerking movements without the tonic phase. These seizures usually affect both sides of the body, last 1 to 2 minutes, and are followed by a period of confusion.
The Root Causes and Brain Locations of Different Seizures
Focal Seizures: Causes and Locations
Focal seizures often result from structural abnormalities such as brain tumors, strokes, or traumatic brain injuries. They can also stem from congenital malformations like cortical dysplasia, vascular lesions, post-infectious scarring, or mesial temporal sclerosis (hippocampal scarring often related to childhood febrile seizures).
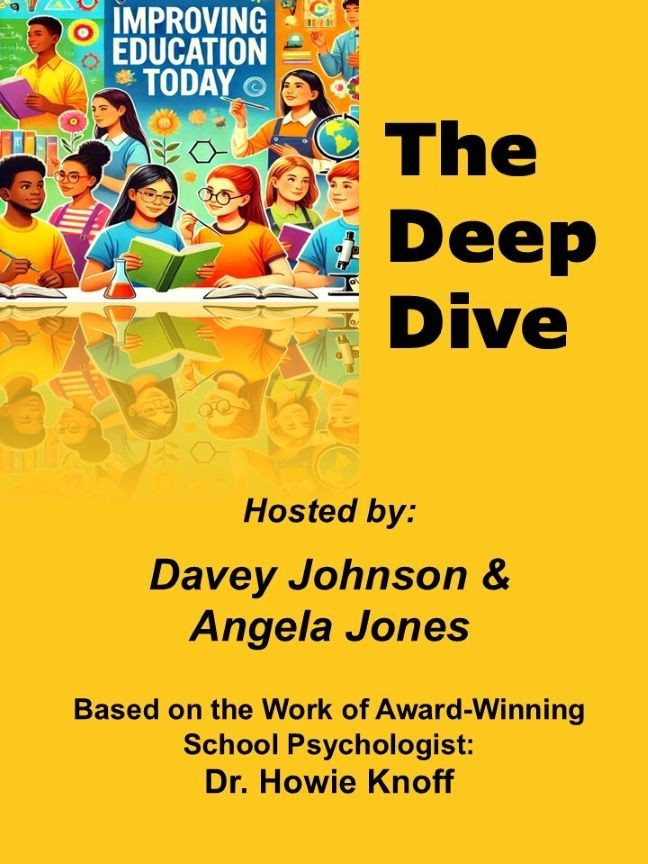
Different brain locations produce different focal seizure symptoms (see Figure below):
- The temporal lobe is the most common location for focal seizures, producing symptoms like déjà vu, unusual smells/tastes, abdominal sensations, and automatisms. Hippocampal involvement is common in temporal lobe epilepsy.
_ _ _ _ _
- The frontal lobe is the second most common location for focal seizures, typically producing bilateral motor movements, vocalization, complex posturing, and hypermotor activity.
_ _ _ _ _
- Focal seizures in the parietal lobe trigger sensory disturbances, with spatial perception issues and numbness or tingling.
_ _ _ _ _
- Focal seizures in the occipital lobe typically cause visual hallucinations, blindness, eye deviation, and blinking.
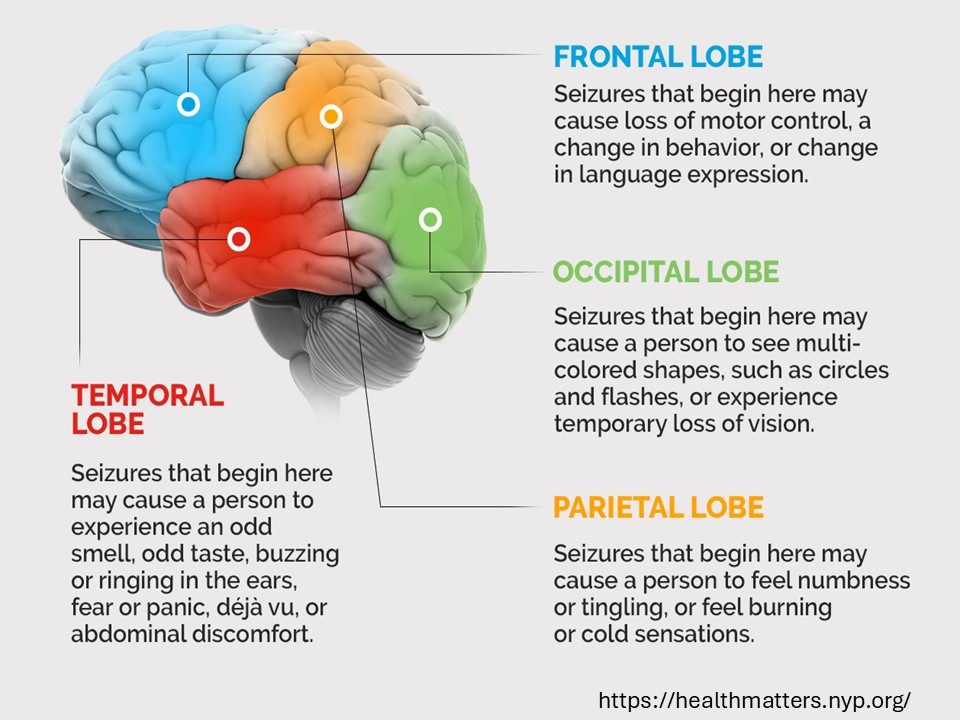
Figure: Major Structures of the Brain Involved in Seizures
_ _ _ _ _
Generalized Seizures: Causes and Locations
Generalized seizures often result from genetic factors like ion channel mutations (such as SCN1A mutations in Dravet syndrome or KCNQ2 mutations), developmental disorders, metabolic abnormalities, synchronization issues between the thalamus and cortex, or neurotransmitter imbalances, especially in Gamma-Aminobutyric Acid (GABA) and glutamate.
Unlike focal seizures, generalized seizures involve both hemispheres from onset. Thalamo-cortical networks are central to most generalized seizures, with the thalamus acting as a relay and synchronization center. Abnormal oscillations between the thalamus and cortex drive many generalized seizures.
Different generalized seizure types have specific origins:
- Absence Seizures are primarily genetic, often involving T-type calcium channel mutations. They stem from abnormal 3 Hz spike-and-wave pattern oscillations in thalamo-cortical circuits, particularly the thalamic reticular nucleus with bilateral cortical involvement.
_ _ _ _ _
- Tonic-Clonic Seizures can have various causes including genetic, structural, metabolic, or unknown factors. They involve widespread cortical activation with brainstem reticular formation involvement, beginning with abnormal firing throughout the cortex and engaging the motor cortex during the convulsive phase.
_ _ _ _ _
- Myoclonic Seizures are often genetic, and they are seen in specific syndromes like Juvenile Myoclonic Epilepsy. They primarily involve the motor cortex and thalamic connections, specifically the precentral gyrus with thalamic modulation.
_ _ _ _ _
- Atonic Seizures are often associated with structural brain abnormalities or genetic disorders, involving sudden inhibition of the motor cortex or interruption of brainstem-spinal pathways.
Special Seizure Types and Conditions: Causes and Locations
Below, we quickly review three additional specialized types of seizures: Febrile and Reflex seizures, and Status Epilepticus.
Febrile Seizures. Febrile seizures represent one of the most common neurological disorders in early childhood, affecting approximately 2 to 5% of children between the ages of 6 months and 5 years. These seizures are characterized by their occurrence during episodes of fever without evidence of intracranial infection or other defined causes.
- Root Causes. The primary trigger for febrile seizures is a rapid rise in body temperature, typically above 100.4°F. This sudden temperature elevation appears more significant than the absolute height of the fever. The child's genetic predisposition plays a substantial role, with a 10 to 20% increased risk among first-degree relatives of affected children.
The immature brain's temperature regulation mechanisms contribute significantly to susceptibility. Young children's brains have not yet developed the robust temperature regulation systems present in adults, making them more vulnerable to temperature-induced neural excitability. This developmental vulnerability explains why febrile seizures predominantly affect children under five years of age and rarely occur in older individuals.
_ _ _ _ _
- Brain Location and Neurophysiology. While febrile seizures are typically exhibited as generalized seizures affecting both hemispheres of the brain, their initiation likely involves temperature-sensitive neurons in the hypothalamus. The hypothalamus serves as the body's thermoregulatory center, and when rapidly rising temperatures overwhelm its capacity to regulate brain temperature, a cascade of events can trigger abnormal neuronal firing.
Research suggests that fever-induced hyperventilation leads to respiratory alkalosis, which increases neuronal excitability. Additionally, inflammatory cytokines released during febrile illnesses may lower the seizure threshold. These factors, combined with the immature brain's limited inhibitory mechanisms, create conditions favorable for seizure generation.
Most febrile seizures resolve spontaneously within minutes and carry an excellent prognosis, with over 97% of children experiencing no long-term neurological consequences.
_ _ _ _ _
Reflex Seizures. Reflex seizures represent a fascinating category of epileptic events triggered by specific sensory stimuli or cognitive activities. Unlike spontaneous seizures, these are consistently provoked by identifiable external or internal triggers.
- Root Causes. The fundamental mechanism underlying reflex seizures involves hypersensitivity in specific sensory cortices. This hypersensitivity creates an abnormally low threshold for neuronal activation in response to particular stimuli. Genetic factors often contribute to this susceptibility, with many reflex epilepsy syndromes showing familial patterns.
The neurophysiological basis involves hyperexcitability in specific neural networks that process particular types of sensory information. When these networks are activated by their corresponding triggers, they may generate synchronized discharges that can either remain localized or spread to involve larger brain regions.
_ _ _ _ _
- Brain Location by Trigger Type
Photosensitive Epilepsy
Initial Location: Visual cortex in the occipital lobe
Mechanism: Flashing lights, contrasting patterns, or specific visual frequencies (typically 15-25 Hz) stimulate hyperexcitable neurons in the visual cortex
Propagation: May remain localized as simple visual phenomena or spread to involve motor areas, resulting in tonic-clonic movements
Demographics: Most common in adolescents, with many patients outgrowing the sensitivity by adulthood
_ _ _ _ _
Audiogenic Seizures
Initial Location: Auditory cortex in the temporal lobe
Mechanism: Specific sounds or frequencies trigger abnormal electrical activity in auditory processing regions
Characteristics: May manifest as auditory hallucinations initially before progressing to motor symptoms if the activity spreads
Notable Examples: Musicogenic epilepsy, where specific musical pieces or genres trigger seizures
_ _ _ _ _
Reading Epilepsy
Initial Location: Language areas in the dominant hemisphere (typically left temporal and frontal regions)
Mechanism: The complex integration of visual processing, language comprehension, and vocalization required for reading overwhelms susceptible neural circuits
Presentation: Often begins with jaw jerking or throat discomfort before potentially generalizing
Cognitive Aspects: Represents an interesting intersection between higher cognitive functions and epileptogenesis
Other notable reflex triggers include eating (temporal lobe), hot water immersion (parietal lobe), and complex activities like mathematics or decision-making (frontal lobe involvement). Treatment approaches typically combine avoidance of triggers with targeted anticonvulsant medications.
_ _ _ _ _
Status Epilepticus. Status epilepticus (SE) represents a neurological emergency characterized by either continuous seizure activity lasting more than 5 minutes or recurrent seizures without recovery of consciousness between episodes. This condition carries significant morbidity and mortality, with mortality rates ranging from 3 to 40% depending on seizure type, duration, age, and comorbidities.
- Root Causes. The fundamental pathophysiology of status epilepticus involves a critical failure of the brain's seizure termination mechanisms. Under normal circumstances, multiple inhibitory processes limit seizure duration. In status epilepticus, these protective mechanisms fail, allowing persistent abnormal electrical activity.
Several specific factors can precipitate status epilepticus:
Medication Withdrawal. Abrupt discontinuation of anticonvulsant medications is a leading cause, particularly in patients with established epilepsy. The sudden removal of inhibitory influences can unleash uncontrolled excitatory activity.
_ _ _ _ _
Acute Brain Injuries. Traumatic brain injury, stroke, hypoxic damage, and central nervous system infections can disrupt normal inhibitory circuits and trigger prolonged seizure activity. These structural lesions may create persistent hyperexcitable foci resistant to normal termination mechanisms.
_ _ _ _ _
Metabolic Disturbances. Severe electrolyte imbalances (particularly sodium, calcium, and glucose abnormalities), uremia, and hepatic encephalopathy can alter the brain's electrical stability. Toxic-metabolic encephalopathies reduce seizure threshold while simultaneously impairing termination mechanisms.
_ _ _ _ _
Progressive Neurological Conditions. Neurodegenerative diseases, brain tumors, and certain autoimmune encephalitides create evolving pathological conditions that can manifest as status epilepticus, particularly in advanced stages.
_ _ _ _ _
- Brain Location and Pathophysiology. The anatomical substrate of status epilepticus depends primarily on the seizure type involved:
Convulsive Status Epilepticus. Involves bilateral cortical regions with prominent motor system involvement. The sustained hyperactivity leads to depletion of inhibitory neurotransmitters, internalization of GABA receptors, and externalization of excitatory NMDA receptors—creating a self-perpetuating cycle.
_ _ _ _ _
Non-Convulsive Status Epilepticus. May involve more limited regions, particularly temporal and frontal networks, without overt motor manifestations. Though less immediately apparent clinically, it can still cause neuronal damage through excitotoxicity.
_ _ _ _ _
Focal Status Epilepticus. Remains confined to specific brain regions corresponding to the underlying pathology, such as stroke, tumor, or focal cortical dysplasia.
_ _ _ _ _
- Progression. The progression of status epilepticus involves multiple pathophysiological stages:
Initial Phase (0-30 minutes). Characterized by excessive neuronal firing with intact compensatory mechanisms, generally responsive to first-line medications
Established Phase (30-60 minutes). Features failing compensatory mechanisms with internalization of inhibitory receptors, increasingly resistant to standard treatments
Refractory Phase (>60 minutes). Demonstrates profound neurochemical alterations, mitochondrial failure, cerebral edema, and systemic complications requiring aggressive intervention.
_ _ _ _ _
Status epilepticus requires immediate medical intervention to prevent permanent neurological damage and life-threatening systemic complications. The longer the duration, the more resistant it becomes to treatment and the greater the risk of adverse outcomes.
Seizures and Their Relationship to Stress and PTSD
Stress and post-traumatic stress disorder (PTSD) can influence seizure activity through complex and bidirectional neurobiological, psychological, and physiological mechanisms. For 30 to 60% of individuals with epilepsy, stress is a significant seizure trigger.
The relationship between stress/PTSD and seizures works both ways. Stress and PTSD can trigger or worsen seizures, while having seizures creates psychological stress, potentially worsening PTSD symptoms. This creates a challenging cycle that requires integrated treatment approaches. Critically, though, while not everyone with stress or PTSD develops seizures, there are established connections that deserve attention.
_ _ _ _ _
Stress affects neurological functioning through several pathways. During stress, the body releases cortisol and other stress hormones that can lower seizure thresholds in susceptible individuals. These hormones affect brain excitability and can disrupt normal electrical activity.
Chronic stress often leads to poor sleep quality, which is a known seizure trigger. Sleep deprivation increases cortical excitability, potentially precipitating seizure activity.
Additionally, acute stress can trigger hyperventilation, leading to changes in blood chemistry that may provoke seizures in predisposed individuals.
_ _ _ _ _
Conversely, seizures themselves can be traumatic events, creating fear and helplessness. The unpredictable nature of seizures creates a sense of vulnerability, and public seizures can lead to embarrassment and social anxiety. The disorientation after seizures can be frightening and traumatic.
This can lead to the development of seizure-related PTSD, characterized by anticipatory anxiety about when the next seizure might occur, intrusive memories or flashbacks to seizure experiences, avoidance behaviors to prevent seizure triggers, and hypervigilance through constant monitoring of bodily sensations for seizure auras. This creates a vicious cycle where stress leads to seizures, which create more stress.
PTSD has been linked to several seizure types. Psychogenic Non-Epileptic Seizures (PNES), also called functional or pseudoseizures (see section below), resemble epileptic seizures but aren't caused by abnormal electrical activity. Studies show 25 to 40% of individuals with PNES have histories of PTSD or trauma. These seizures often manifest with convulsions, altered awareness, and emotional disturbances.
PTSD-specific factors include the persistent hypervigilance state that keeps the brain in a heightened state of excitability, sleep disruptions that independently lower seizure threshold, and flashbacks that trigger acute stress responses potentially precipitating seizures.
In people with epilepsy, PTSD and chronic stress can lower seizure thresholds, potentially triggering focal seizures (affecting one brain area) or generalized seizures (affecting both hemispheres). Dissociative seizures are psychological in nature and often connected to trauma processing. They can include altered awareness, motor symptoms, and sensory disturbances.
The connection between stress, PTSD, and seizures highlights the importance of integrated, multidisciplinary treatment approaches that address both neurological and psychological factors. School professionals are instrumental both in this integration and in some areas of treatment.
PTSD or Stress-Induced Psychogenic Non-Epileptic Pseudoseizures
As introduced above, Psychogenic Non-Epileptic Seizures (PNES), formerly known as "pseudoseizures," are episodes that resemble epileptic seizures, but without the corresponding EEG activity. About 50 to 80% of PNES patients report significant trauma or abuse histories, and PNES is significantly more common in people with PTSD.
As discussed in Part II of this Blog Series, PTSD creates profound changes in brain function, particularly in regions responsible for regulating the stress response. The amygdala, hippocampus, and prefrontal cortex—areas critically involved in fear processing and emotional regulation—often show altered activity patterns and even structural changes in individuals with PTSD.
These neurobiological alterations can create a heightened state of physiological arousal that, in some cases, manifests as seizure-like episodes. However, unlike epileptic seizures, which stem from abnormal electrical activity in the brain, PTSD-induced seizures typically represent the brain's response to overwhelming emotional triggers or trauma recollections.
As such, PNES are often triggered by emotional events or conflicts, and they typically develop gradually rather than suddenly. They may fluctuate in intensity, show asynchronous movements that are out of phase or inconsistent, and the individual’s eyes are often closed during the events—contrary to most epileptic seizures.
Critically, the neuro-biological processes involved in some of the seizures discussed earlier in this Blog and PNES-pseudoseizures are similar. Similarly, as discussed in Part II of this Blog Series, these same neuro-biological processes also occur for some migraines.
Thus, these three triangulated events (migraines, seizures, and pseudoseizures due to stress or PTSD) need to be medically and psychologically differentiated. This is especially important as schools need to know what involved students are actually experiencing, and the most effective ways to medically and psychoeducationally respond.
In contrast to epileptic seizures, individuals experiencing PNES-pseudoseizures may respond to verbal stimuli during events, and they typically recover quickly and without the confusion period common (after epileptic seizures). Finally, PNES episodes often last longer than typical epileptic seizures (i.e., greater than 2 minutes).
Importantly, patients with PNES are not faking or consciously producing their symptoms. The distress and disability caused by PNES is very real, and about 10 to 30% of patients with PNES also have epilepsy, complicating diagnosis.
_ _ _ _ _
Recognizing the Symptoms
A common symptom of PTSD-induced pseudoseizures includes uncontrollable shaking or trembling of the body, which may affect the entire body or be localized to specific areas. Unlike epileptic seizures, individuals are conscious and aware of their surroundings during PNES events—even though they may not be responsive. Individuals also report feeling detached or "foggy" during PNES episodes, rather than being completely unconscious.
Other physical symptoms often include rapid breathing, increased heart rate, sweating, and sensory disturbances. Some individuals report unusual sensations such as tingling, numbness, or visual distortions before or during episodes.
Perhaps most distinctively—as noted earlier, individuals with PTSD- or stress-induced pseudoseizures typically don't show the characteristic brain activity patterns seen in epileptic seizures when monitored with EEG testing.
_ _ _ _ _
Underlying Causes and Risk Factors
Several factors contribute to the development of PTSD-induced pseudoseizures. For example, the severity and duration of trauma exposure significantly impact the likelihood of developing pseudoseizures. Individuals who have experienced prolonged or repeated trauma—such as survivors of child abuse or victims of domestic violence—appear to be at higher risk.
Research also suggests that certain pre-existing conditions may increase susceptibility. These include prior traumatic brain injuries, history of childhood seizures, and genetic factors influencing stress response regulation.
Social and psychological factors also play important roles. Limited support systems, ongoing life stressors, and comorbid conditions like depression or substance use disorders can exacerbate both PTSD symptoms and pseudoseizure occurrence.
_ _ _ _ _
Treatment Approaches: A Multi-Faceted Strategy
Effective management of PTSD-induced pseudoseizures requires a comprehensive approach addressing both neurological and psychological aspects of the condition:
- Psychotherapy. Trauma-focused cognitive behavioral therapy (TF-CBT) remains a cornerstone of treatment. By processing traumatic memories and developing healthy coping mechanisms, patients can reduce the emotional charge that triggers seizure activity. EMDR (Eye Movement Desensitization and Reprocessing) has shown particular promise in addressing both PTSD symptoms and reducing seizure frequency by helping the brain process traumatic memories.
_ _ _ _ _
- Medication Management. While traditional anti-seizure medications may not be effective for PTSD-induced seizures, other pharmacological approaches can help. Selective serotonin reuptake inhibitors (SSRIs) and other antidepressants can regulate the stress response system and improve overall PTSD symptomatology. In some cases, anxiolytic medications may be prescribed for short-term use during periods of acute stress.
_ _ _ _ _
- Relaxation Training. Biofeedback and progressive muscle relaxation training can help individuals recognize early warning signs of PNES events, using these strategies to prevent or minimize episodes. Regular practice of these methods helps regulate the autonomic nervous system, potentially reducing seizure frequency and severity.
_ _ _ _ _
- Comprehensive Care Coordination. The complex nature of PTSD-induced pseudoseizures necessitates collaboration between neurologists, psychiatrists, psychologists, and other healthcare providers. This team approach ensures that both neurological and psychological aspects of the condition receive appropriate attention.
_ _ _ _ _
The Importance of Awareness and Support
Despite growing understanding of PTSD-induced pseudoseizures, many individuals still face significant challenges in receiving appropriate diagnosis and treatment. Misdiagnosis as epilepsy or dismissal of symptoms as "just psychological" remains common. Raising awareness among healthcare providers, educators, and the general public about this legitimate neuropsychiatric condition is essential.
For students living with PTSD-induced pseudoseizures, supportive educators and in-house related services professionals can make a tremendous difference. These students need validation and support, practical coping strategies—and the permission to use them, and the comfort of knowing that they are not alone in this experience.
The Connection Between Seizures and Traumatic Brain Injuries
Traumatic brain injury (TBI) and concussions share a significant relationship with seizures, with the connection varying based on injury severity, location, and individual factors.
Post-traumatic seizures (PTS) are classified based on when they occur relative to the injury:
- Immediate/Impact Seizures occur at the moment of impact and are relatively rare, seen in approximately 1 to 4% of TBI cases. They are not strongly associated with the development of post-traumatic epilepsy.
_ _ _ _ _
- Early Post-Traumatic Seizures occur within 7 days of injury. Their incidence ranges from 1 to 4% in mild TBI to 10 to 25% in severe TBI. These represent an acute reaction to injury rather than epilepsy.
_ _ _ _ _
- Late Post-Traumatic Seizures occur beyond 7 days after injury and are often considered diagnostic of post-traumatic epilepsy. Their incidence ranges from less than 5% in mild TBI to 10 to 50% in severe TBI, depending on specific risk factors.
_ _ _ _ _
Post-Traumatic Epilepsy (PTE)
Post-traumatic epilepsy refers to recurrent seizures that develop as a chronic condition following TBI. The risk varies based on TBI severity:
- Mild TBI/Concussion generally presents a low risk (approximately 1 to 2%), though the risk may be higher with multiple concussions. This connection is often overlooked in cases of multiple mild TBIs.
_ _ _ _ _
- Moderate TBI carries approximately 2 to 4% risk within 5 years, increasing with specific injury characteristics.
_ _ _ _ _
- Severe TBI presents up to 15 to 20% risk of developing epilepsy, with risk remaining elevated for at least 10 years post-injury. The highest risk occurs in penetrating injuries (up to 50%).
_ _ _ _ _
Risk Factors and Mechanisms
Several factors increase the risk of developing PTE:
- Injury-related factors include penetrating injuries (especially with dural penetration), intracranial hemorrhage (particularly subarachnoid and subdural), brain contusions (especially in frontal and temporal regions), depressed skull fractures requiring surgical elevation, early post-traumatic seizures, loss of consciousness greater than 24 hours, and a Glasgow Coma Scale less than 10.
_ _ _ _ _
- Patient factors that include age (higher risk in very young children and adults over 65), genetic predisposition, pre-existing brain pathology, and alcohol use.
_ _ _ _ _
The development of seizures after TBI involves multiple mechanisms that evolve over time:
- In the acute phase (minutes to days), altered neurotransmitter release, ion channel dysfunction, blood-brain barrier disruption, and cerebral edema play key roles.
_ _ _ _ _
- During the subacute phase (days to weeks), neuroinflammation, free radical production, axonal injury, and altered cerebral blood flow become important factors.
_ _ _ _ _
- In the chronic phase (months to years), neuronal circuit reorganization, gliosis, changes in inhibitory circuits, blood-brain barrier alterations, and altered gene expression contribute to seizure development.
Management Approaches for Different Types of Seizures
For PNES and Stress-Related Seizures
Psychological interventions like Cognitive Behavioral Therapy (CBT), progressive relaxation therapy and other stress reduction techniques, trauma-focused therapy like Eye Movement Desensitization and Reprocessing (EMDR), and biofeedback can be effective for both PTSD and seizure management.
Medical interventions utilizing selective anti-seizure medications are appropriate and should be prescribed and monitored by the individual’s primary care or specialization physician. Care must be taken as some medications may lower seizure threshold, or complicate long-term resolution.
Lifestyle modifications are crucial, including prioritizing regular, quality sleep, implementing stress management routines (regular exercise, relaxation techniques, breathing exercises), keeping seizure diaries with stress ratings to identify personal patterns, and joining support groups.
_ _ _ _ _
For Post-Traumatic Seizures and Epilepsy
Acute seizure preventative or active treatment often involves anti-seizure medications for seven days after moderate-severe TBI. However, many of the common treatment medications have limited effectiveness in preventing long-term epilepsy development.
For established PTE, medications like levetiracetam, carbamazepine, and lamotrigine are commonly used. Surgical options exist for medication-resistant focal epilepsy with an identifiable seizure focus, and neuromodulation techniques like VNS (Vagus Nerve Stimulation) can help selected cases.
School Support and Seizure Management Approaches
Schools play a crucial role in ensuring the safety, academic, and social success of students with epilepsy. Many states have passed laws requiring schools to provide seizure recognition and first-aid training for staff, maintain Seizure Action Plans for affected students, and administer prescribed medications when necessary. Programs like “Seizure Training for School Personnel” (see references for this and others below) provide educators, nurses, and staff with essential knowledge on seizure types, first aid, and emergency response.
More specifically, schools can take several steps to ensure the safety and well-being of students with epilepsy and seizure disorders. Some key strategies include:
- Close communication with the affected parents and the students themselves—as well as their designated medical specialists—regarding seizure-prevention, immediate response, and post-seizure actions and activities to address both medical and safety concerns.
Much of this should be coordinated by the administration and the School Nurse, as well as selected members of the school’s Multi-Tiered Services Team.
Schools ensure that nurses and other personnel are trained and available to administer rescue medications and monitor students with frequent seizures.
_ _ _ _ _
- Communication with and training for school staff (including bus drivers, paraprofessionals, recess and lunchroom aides, and necessary others) who are likely to be present during a seizure event.
_ _ _ _ _
- Communication with and awareness training for students who are likely to be present during a seizure event—including any anti-teasing or bullying discussions and plans needed (to reduce the stigma sometimes associated with seizures and to provide active support to affected students).
Some schools incorporate epilepsy education into their health curricula even when there are not affected students in the student body.
_ _ _ _ _
- Determination as to whether the student qualifies for a 504 or Individualized Education Plan, respectively—or at least a Seizure Action Plan. These plans help address not just the medical preparations needed, but also the academic, social-behavioral, and related services needed by the student.
These plans should also include any accommodations, as well as therapy services needed (e.g., occupational therapy, cognitive-behavioral or relaxation therapy).
In addition, specific school staff may be designated to help students adhere to medication schedules and administer emergency treatments when needed.
_ _ _ _ _
- Seizure Action Plans (on their own or embedded in one of the other plans referenced above) should outline first aid steps, seizure triggers, emergency procedures and contacts, and medication protocols.
_ _ _ _ _
Sample Successful School Seizure Safety Programs
Seizure Safe Schools Initiative. Led by the Epilepsy Foundation, this nationwide effort is dedicated to passing legislation that ensures that schools provide seizure recognition and first-aid training for staff, maintain Seizure Action Plans, and administer prescribed medications. Over half of U.S. states have adopted some form of this legislation.
www.epilepsy.com/advocacy/priorities/seizure-safe-schools
_ _ _ _ _
Seizure Management in Schools. The American Academy of Pediatrics provides best practices for school-based seizure management, including identifying students with epilepsy, training staff, and ensuring proper documentation and emergency response protocols.
_ _ _ _ _
Seizure Preparedness Programs. The Epilepsy Foundation offers training for school personnel, including teachers, nurses, and administrators, to improve seizure response and create a supportive environment for students with epilepsy.
www.epilepsy.com/preparedness-safety/schools
_ _ _ _ _ _ _ _ _ _ _ _
Summary
This three-part Blog Series has focused broadly on three clusters of biologically-based conditions and their impact on students’ academic and/or social, emotional, or behavioral learning, interactions, and success.
Throughout the Series, we have stressed how important it is for the different multi-disciplinary experts on every school’s 504, IDEA, or MTSS (Multi-Tiered System of Supports) team—as well as teachers and others—to understand how these biological conditions connect to curriculum, instruction, and learning, as well as to needed assessments, accommodations, and interventions.
Part I of this Blog Series noted that virtually all of the disabilities that qualify students for services under Section 504 of the Rehabilitation Act of 1973 or the Individuals with Disabilities Act (IDEA, 2004), respectfully, have an important relationship to these students’ biological, physical or physiological, biochemical, or neuropsychological functioning. We then provided a primer on students’ vision, hearing, and respiratory/nasal functioning—specifically, how to screen and identify different problems in each area; and how these problems can significantly affect student learning, socialization, and functioning in the classroom.
In the second Blog, we initially distinguished between headaches and migraines, and described how migraines affect students academically and socially in school. We then discussed four types of migraines: Ocular/Retinal, Vestibular, Concussion-related, and Stress or Post-Traumatic Stress Syndrome migraines—addressing their (a) common neurological, limbic, and biochemical structures and pathways; and (b) their distinct clinical presentations, neurobiological mechanisms, diagnostic considerations, and management approaches.
In this third Blog, we discussed the types and impact of seizures on students’ learning and engagement in school. This Blog provided detailed information in the following sections:
- An introduction to seizures with general characteristics, incidence levels, and their impact on students in school
- The different types of seizures—including three types of more-specialized seizures—with their specific characteristics and physical manifestations
- The neurological root causes for each type of seizure discussed, along with the areas of the brain involved
- Seizures and their relationship to stress and PTSD
- The link between PTSD and Psychogenic Non-Epileptic Seizures (PNES), also called functional or pseudoseizures, including their symptoms, underlying causes and risk factors, treatment approaches, and the support these students need in school
- The connection between seizures and traumatic brain injuries or concussions
- Management approaches for different types of seizures
- Specific school support and seizure management approaches
_ _ _ _ _
Understanding the various types of seizures and their complex relationships with stress, trauma, and brain injury is crucial for proper diagnosis, treatment, and support. The bidirectional relationship between seizures and psychological factors highlights the importance of integrated care approaches that address both the neurological and psychological aspects of these conditions.
All of this is important for school staff who have affected students in their classrooms, common schools areas, on school buses, and participating in extra-curricular activities. While seizures can be frightening to witness or experience, most can be effectively managed with proper medical care and planning by school personnel.
School staff need to remember that seizures are also frightening to the students directly experiencing them (especially younger students), and to students (and staff) who witness an event. Seizure first aid primarily involves ensuring safety during the event and being a calm, supportive presence. Knowing the specific type of seizure someone experiences can help educators coordinate with parents, the students involved, and other healthcare providers to ensure that everyone is “on the same page,” responding to events correctly, and providing services and supports with integrity.
_ _ _ _ _
The “Improving Education Today” Podcast: A New Professional Development Resource Complementing this Blog
This past January, we announced a new partnership and resource for you.
The partnership is with popular AI Educators, Davey Johnson and Angela Jones. . . and the resource is their Podcast:
Improving Education Today: The Deep Dive
For each published bimonthly Blog, Davey and Angela summarize and analyze the Blog in their free-wheeling and “no-holds-barred” Podcast. . . addressing the topic’s importance to “education today,” and discussing their recommendations on how to apply the information so that all students, staff, and schools benefit.
You can find the Podcast that accompanies this Blog message at the following link:
Improving Education Today: The Deep Dive | Podcast on Spotify
Davey and Angela have also created a Podcast Archive consisting of all of this year’s Blog (Volume 3), as well as those from 2024 (Volume 2), and 2023 (Volume 1).
The Podcasts are posted on Spotify, and you can “Follow” the Podcast Series so that you will be automatically notified whenever a new Podcast is posted.
Many districts and schools are using the Podcasts in their Leadership Teams and/or PLCs to keep everyone abreast of new issues and research in education, and to stimulate important discussions and decisions regarding the best ways to enhance student, staff, and school outcomes.
If you would like to follow this Blog or a Podcast up with a free one-hour consultation with me, just contact me and we will get it on our schedules.
I hope to hear from you soon.
Best,
Howie
[To listen to a synopsis and analysis of this Blog on the “Improving Education Today: The Deep Dive” podcast on Spotify: CLICK HERE]